Indian Journal of Physiology
and Pharmacology
and Pharmacology
Indian Journal of Physiology and Pharmacology |
 (252x320).jpg) |
Volume 58 - Number 2 April - 2014 (Current issue) ISSN 0019-5499 |
Mid-latency Auditory Evoked Potential Response Revealed as an Evidence of Neural Plasticity in Blind IndividualsAnbarasi Muthusamy, Rajkumar Gajendran and Vishwanatha Rao B. |
There is a general impression that visually blind individuals show an exceptionally better perception of other sensory modalities such as hearing, touch and smell sensations. In this study, we intended to compare the mid-latency auditory evoked potential response (MLAEP) or Middle latency Response (MLR) to get an idea of the activity pattern of auditory thalamus and cortex between 30 visually handicapped subjects and 30 normal sighted subjects. The results showed a decrease in many of the MLR wave latencies, but highly significant for the wave Pa (P value <0.002). This fact can be reflected as an evidence of existence of crossmodal neuroplasticity. We also inferred that there are significant gender differences with latencies shorter in males than females (P value <0.02) in the blind subjects group which could be attributed to their rehabilitation training. |
Neuroplasticity is the capacity of the nervous system
to reorganize itself as a consequence of normal
development and maturation, during learning process,
after damage to the nervous system or as a result
of sensory deprivation (1). Cross modal plasticity
is the neuroplasticity occurring as an adaptive
mechanism to compensate for lost function and/or
to maximize the remaining functions in the event of brain injury (2). There are number of studies providing
experimental evidences for this compensatory
plasticity in blind humans (3, 4, 5, 6). The younger
the age of onset of blindness, the more plasticity
the visual cortex seems to have (7). Such plastic
changes vary widely across brain systems, giving
rise to highly specific alterations as a function of
the nature of altered experience, its timing and brain
systems involved. Thus the possible mechanisms of
cross-modal plasticity may be changes in the
subcortical connectivity like in brainstem and
thalamus or changes in the cortico-cortical feedback
or in the long-range connections between the primary
cortices (1). But these sensory changes seem to be
driven by experience from peripheral activity rather
than blindness per se. In our previous study (8), we
recorded significantly shorter latency of wave V of
Brainstem evoked response audiometry (BERA) in
blind individuals when compared to the normal sighted subjects. The generators of BERA waves include
Wave I and II from Cochlear Nerve and Nuclei, Wave
III from Superior olivary nucleus, Wave IV from Lateral
lemniscus and wave V from Inferior colliculus (9). In
this study, we intended to compare the Mid-latency
auditory evoked potential response (MLAEP) or
Middle latency response (MLR) in blind subjects with
that of normal sighted subjects. MLR is the transient
response that occurs in the 10 to 50 milliseconds
post-stimulus time period. The generators of MLR
are located in the auditory thalamus ie. Medial
geniculate body, Heschl gyrus (auditory cortex) and
the thalamo-cortical projection areas (10). The various
waveforms of MLR are No, Po, Na and Pa, out of
which the wave Pa (also called P30), which is the
positive peak occurring usually at 30 to 36
milliseconds post-stimulus period is of much clinical
use. We studied the differences in the peak latencies
and amplitude of Na-Pa wave between blind and
normal sighted subjects. |
Type of study This is a comparative, cross-sectional study done in Institute of Physiology and Experimental Medicine, Madras Medical College, Chennai. The study was approved by the Institutional Ethical Committee (Ref:L.Dis.No.3798/P&D3/Ethics/GGH). Subject selection The study group consisted of 30 blind students (15 male and 15 female) of age ranging from 17 to 23 years, recruited from "The Blind student's Graduate Association, Chennai" after getting informed and written consent. The mode of training for these students since their school hood period is Braille Method and auditory stimulation using audio cassettes. Students with any auditory pathology, known diabetes, long duration of anemia, mental retardation and those taking long term medications that may affect hearing are excluded from the study. Control group consisted of 30 age and sex matched students with normal vision who were in I, II and III year of MBBS. Same exclusion criteria were followed for the control group. Methodology The entire procedure was divided into history taking, examination of systems & ENT and recording of evoked potentials. It was done in the day time from 9.00 AM to 4.00 PM in the departments of ENT and Physiology. History regarding the general details like name, age and address of the subjects, their educational status with mode of training, cause and duration of blindness, family history of blindness, auditory problems, diabetes mellitus and other co-morbid conditions were elicited in the study group subjects. Similar history except for details on blindness was elicited in control group subjects. Instead, they were enquired about any visual problems like refractive error. Regular anthropometric measurements (height and weight) were taken in both groups. General physical examination, examination of cardiovascular system, respiratory system and central nervous system were done in both groups. Both the group subjects were then evaluated for any ENT pathology by tuning fork tests and otoscopic examination. If there was presence of wax, it was promptly dissolved by appropriate treatment. Recording of evoked potentials – VEP and MLR Both the groups of subjects were subjected to VEP and MLR. The apparatus used in our study is RMS EMG EP MARK II. The apparatus is set up as per the "Recommended standards for the clinical practice of Evoked Potentials" introduced in Guideline 9A: Guidelines on Evoked Potential, by American Society of Clinical Neurophysiology (11). The evoked potentials were recorded in a closed dark room free from external noise. The temperature of the room was maintained at 23°C–24°C throughout the procedure. Assessment of vision by VEP The subjects of the study group showed absence of perception of hand movements and perception of light. In addition, blindness was confirmed by absent Visual Evoked Potential (VEP) responses. In the control group, visual acuity and VEP were done to ensure normal vision. The latency of P100 wave of VEP of the subjects of control group was found to be within normal limits. Recording of middle latency response The electrical montage used for testing is L: Cz-A1, R: Cz-A2, Ground: Fz. The nature of the stimulus to the test ear is a broad band click of 100 μs duration with the intensity of 85 dB at a stimulus rate of 11.1 clicks per second. The analysis time was set as 50 ms and included 1500 trials with two repetitions. The contra lateral ear was masked with white noise of 50-60 dB. The wave peaks of MLR namely, No (negative wave at around 10 ms), Po (positive wave at 10-15 ms), Na ((negative wave at 16-30 ms) and Pa (positive wave at 25-45 ms) were recorded (10). The amplitude of wave Na-Pa was also noted. Since the myogenic potentials offer a considerable contamination of MLR potentials, the subject is seated comfortably with neck completely relaxed. Statistical analysis of data Statistical analysis was done using SPSS version 16.0. The demographic data were statistically analyzed using one-way ANOVA. The results of MLR were analyzed using Student's independent T test. P value of <0.05 is considered to be statistically significant. |
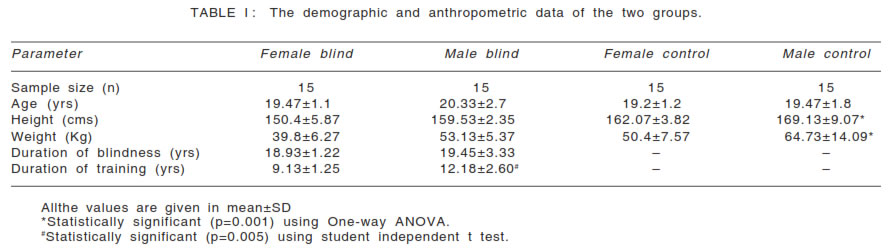
The demographic data, anthropometric data and details on the duration of blindness and peripheral training of blind subjects are given in Table I. Table II shows the latencies and amplitude of MLR
waveforms of all the subjects. On analysing the
gender differences, in the study group, the latencies
of waves Po and Na are significantly decreased in
both ears with P value of 0.02 in the right ear and
0.003 in the felt ear for the wave Po and p value of
0.0001 for the wave Na in both ears. However, in the control group, no such significant differences are
observed. |
 |
 |
 |
On comparing the wave latencies between study and control groups (Fig. 2), the latencies of waves Po, Na and Pa are significantly reduced in the male study group (p values for right ear : Po - 0.03, Na - 0.003 and Pa -0.0001 and left ear: Na - 0.05 and Pa -0.001). Comparison of female study group with control group showed a highly significant decrease in the latency of the wave Pa (P value - 0.002 in the right ear and 0.001 in the left ear). The amplitude of Na-Pa wave on analysis was not
statistically significant when compared between the
study and control groups and also between male
and female subjects. |
Neuroplasticity is the life-long ability of the brain to reorganize neural pathways based on new experiences. It can be a normal process of learning and memory or may occur to compensate for a lost sensory function. The latter is coined as 'Cross-modal plasticity'. These neuroplasticity changes usually involve neurons in the cortical level and its corticocortical connections. But it may also involve the subcortical centers and their connecting tracts (1). In this study, we intended to relate the neuroplastic changes using Mid-latency response of auditory evoked potential as a tool between the blind and normal sighted subjects and also between both the genders. On observing the demographic and anthropometric parameters (Table I), we observed there is significant difference (p value <0.001) in the height and weight of study group when compared to control group. This may be due to the differences in the socio-economic status between the subjects chosen. Duration of blindness and peripheral training The average duration of blindness was slightly higher in males, but was not statistically significant. Also, in all the subjects, blindness was due to peripheral damage of the visual system and there were no additional neurological problems. Kujala T et al. (12) have also demonstrated in their study that plastic changes in neural populations involved in processing of auditory space following early loss of vision. Animal research by Volgyi et al. (13) had documented that the compensatory effect was much greater if deprivation occurred early in life. Grunewald et al. (14) had stated that during a sensitive period of early postnatal development extensive remodeling occurs in the blind via a succession of local synaptic changes. In support of this theory, auditory responses seem to depend on duration of sensory loss, experience and training. In our study, we have selected the subjects of the study group such that their average duration of blindness would be optimum to produce the plasticity changes, if any. Activation of the new functional connections of blind subjects is strongly task-related and training–induced (15). Synapses are dynamic structures, increasing and decreasing in their complexity and number with use and experience. The amount of blood flow and expression of molecules essential for the cortical development also depends on the activity of the particular neurons (16). The explanation of the cortical representation occurring in blind appears to be that, cortical connections of sensory units have extensive convergence and divergence with connections that can become weak with disuse and strong with use. Diana M. Kahn & Leah Krubitzer (2) in their study have postulated that the amount of cortical reorganization is greatly modified by peripheral innervations and activity patterns generated with use. A number of studies in adult mammalian neocortex also support this issue. In our study group, the mean duration of peripheral training (Braille method/auditory training) was 9.13+1.25 yrs in females and 12.18+2.6 years in males. The duration of training was significantly higher in males (p=0.005) which may be because of earlier rehabilitation training given to males. Gender differences Elena Amenedo and Fernando Dfaz (17) in their study
showed that Pa latency was longer in males when
compared to females. Another study by Tucker et al
(18) also showed that Pa latencies were longer in
male subjects, and Pa amplitudes were larger in
female subjects. But our study has contradicted the
above studies that males have shorter latencies of
waves Po and Na, but only in the study group. The
control group does not show any difference. We can attribute this inference to the significantly increased
duration of peripheral training that the blind males
have undergone. Thomas Elbert et al. (19), in their
comparative study in blind and normal sighted
individuals have found that 'the development of usedependent
cortical reorganization may be a
consequence
of the absence of visual input in Comparison of MLR waveforms between study and control groups A study on trained blind students done by N. K. Manjunath et al. (20) inferred that the peak latencies of the wave Pa and Nb were significantly reduced in congenitally blind subjects. Another study by Naveen et al. (21) have found that the Na and Pa middle latency auditory evoked potentials (MLAEP) were not significantly different in congenitally blind subjects when compared with the same values in normal sighted subjects but the Nb component of MLAEP had a significantly shorter latency in congenitally blind persons. No studies compared the wave latencies of No, Po and Na waves of MLR. It is apparent from our study that the blind students showed significantly shorter wave latencies for waves Po, Na and Pa among males and for the wave Pa among females. Since the wave Pa is the most consistent of all the MLR waves, significant reduction in the latency of wave Pa is strongly an evidence of improved auditory activity in the study group subjects. The generator of the wave Pa is the dorso-medial part of Heschl gyrus. This proves that processing at this neural level occurs more efficiently in the blind. Since our study also showed a significant reduction in the No, Po and Na in males, the areas of medial geniculate body and polysensory nuclei of the thalamus which were the generators of these waves were also found to be increasingly active in blind subjects. Conclusion From our study it is evident that the blind subjects have enhanced attention and perception mechanisms compared to normal sighted subjects. Also the significant shorter latencies of MLR waves in male subjects of our study group suggest that the peripheral enhancement training makes a positive role in the increased auditory performance of blind people. This implies that sensory substitution prostheses can be developed based on these additional neural resources to perform tasks that partially compensate for the loss of vision. Lacunae in this study
Future research
|
|